
I have coached many people who had unnecessary anti-reflux surgeries performed. For example, I had one client in his mid 20’s that was suffering from upper gut dysbiosis (likely H. pylori) that had what I consider to be an unnecessary Nissen fundoplication performed. He was suffering from ulcers, gastritis, and reflux that was uncontrolled even after the surgery. His doctor refused to believe H. pylori was the cause of his issues because his test was negative for it, yet he had all the hallmark symptoms. Two weeks following an upper gut antimicrobial protocol, all of his symptoms disappeared. There was no need for him to have a Nissen fundoplication, and he would either have another surgery to reverse it or live with it for the rest of his life, which both have associated risks. So why does Fix Your Gut only rarely recommend anti-reflux surgeries, after all, available avenues have been exhausted? Which anti-reflux surgery is best if you have to have one performed? Finally, how do you obtain relief from reflux before surgery, so it does not have to be performed?
Nissen Fundoplication
A Nissen fundoplication is a rarely needed and harmful laparoscopic surgery, in my opinion for people suffering from reflux disorders. When a person has the Nissen procedure performed they have the top part of the stomach (gastric fundus) stapled around the lower esophageal sphincter (LES) or, the lower part of the esophagus so that it is strengthened and reflux into the esophagus is blocked. Dr. Rudolph Nissen performed the first Nissen fundoplication in 1955.1 Like other conventional GERD treatments; this seems like a great idea in theory. The main cited study of Nissen surgical success rates shows that 73% (after ten years) of people that have had the surgery are “cured” of their reflux disorders (out of a tiny sample size of 249 people), which is a great thing, right? 2
But the problem with gastrointestinal reflux surgeries is that most people who have had them are now left with a host of other issues, some not reversible. Some of the complications include:3
- Reflux and regurgitation (known as Nissen surgical failure, yes I know the surgery is supposed to prevent it, but for many it does not)
- “Gas” bloat syndrome
- Delayed gastric emptying (vagus nerve damage)
- Gastroparesis
- Weight loss
- Dysphagia
- Abdominal adhesions
- Difficult or absent ability to vomit
- Gastric dumping syndrome
- Gastic cardia (Roemheld) syndrome
- Early fullness (satiety)
- Dysautonomia (may only worsen)
- Chest pain
- Death during or from surgical complications (one to two percent possibility per studies)
A Nissen fundoplication can also become undone over time and occurs on average in about 10% of the people that have had the surgery, requiring it to be redone.4 “Gas” bloat syndrome is a syndrome where the stomach cannot correctly expel gas through burping. In some extreme cases of “gas” bloat syndrome, you may not be able to even burp or vomit at all when needed, which can cause intense pain and distress. “Gas” bloat syndrome has about a 41% occurrence rate in people who have had a Nissen procedure and for some the condition it may relieve itself within two months; occasionally some people continue to suffer from it until the Nissen is either redone or reversed.5 Gastric dumping syndrome rarely occurs from the procedure, and occurs when the stomach dumps its contents into the duodenum before complete digestion has taken place. Gastric dumping syndrome can cause duodenal inflammation, diarrhea, weight loss, malnutrition, and hypoglycemia.6 Since the Nissen procedure does not relieve the underlying problem causing the reflux which for most is upper gut dysbiosis their reflux disorders eventually come back within a few months or years as consistent pressure from bloating weakens the Nissen over time. Finally, a friend of mine joined an anti-reflux surgery group on Facebook and has been sending me comments of people that have regretted getting the surgery. He has sent me hundreds if not thousands over many years. Having a Nissen fundoplication performed should be avoided at all costs!
“The incidence of postoperative failure is 2 to 30%. The frequency of post-fundoplication paraesophageal hernia is 7% and reoperation may be necessary if clinical response is not good. Reoperation frequency is 4 to 9%, but the fact that postoperative dysphagia is very high (33%) must be taken into consideration. Ascending migration of the fundoplication towards the thorax can be progressive and life-threatening for the patient. Other authors have reported reintervention rates of 1.8 to 10.8% for persistent dysphagia“7
What about the TIF prodcedure, Is It Any Better Than Having a Nissen Fundoplication?
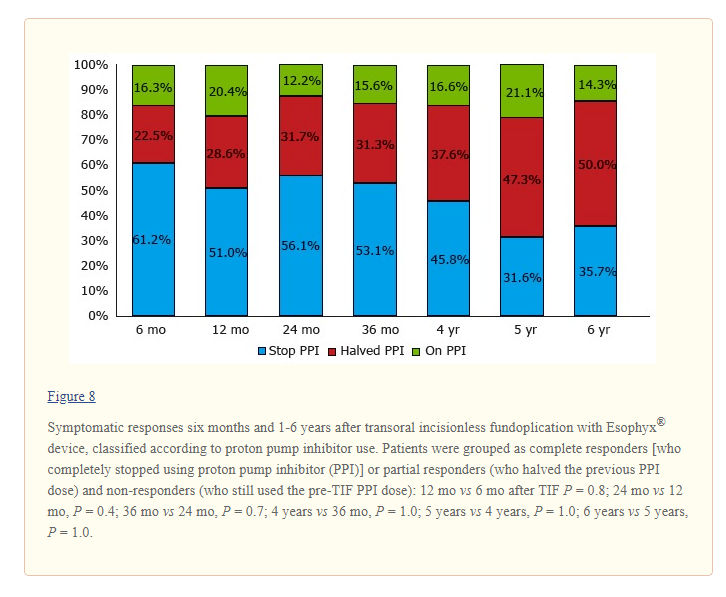
The transoral incisionless fundoplication or TIF procedure is different than a traditional Nissen in that it does not require any incision to perform the fundoplication. The TIF procedure was approved by the United States Food and Drug administration in 2007 for the treatment of GERD. TIF is an endoscopic technique performed using the EsophyX device which an endoscope and a tissue retractor are placed down the esophagus through the oral cavity. The tissue retractor creates a full-thickness serosa-serosa plication at the Z-line where the LES is located. The procedure, performed under general anesthesia in an endoscopy room, constructs a valve three to five centimeters in length and 200 to 300 degrees in circumference using fasteners. If you have a hiatal hernia suction can be applied by the device to pull the stomach downwards, correcting the stomach’s anatomical position. Additionally, TIF is an outpatient procedure, performed by a gastroenterologist or surgeon in an endoscopy room, and should not take more than sixty minutes to complete.8 9 10
If there is no other choice and you had to get a fundoplication, this is the procedure I reluctantly recommend. The TIF procedure appears to cause less scarring than a Nissen fundoplication, and recovery rates seems to be better because of the less invasive surgery being performed. Studies have shown that approximately 3% to 10% of patients who undergo TIF will experience an adverse event. Some of the more concerning side effects of TIF include a mucosal tear, perforation, bleeding, pneumothorax, and mediastinal abscess. However, the serious side effects are rare and are also seen in any LES strengthening surgery. With the TIF procedure the chance of developing gas bloat syndrome is reduced or eliminated compared to a standard fundoplication, and the chances of the TIF becoming undone are lower. TIF like most LES strengthening procedures does not last forever because it does not correct the underlying problem for most, which is upper gut dysbiosis, so reflux does reoccur for most eventually in some degree of severity. Finally, I recommend the newer TIF-2 procedure performed (again if you must) which is a modification of the TIF-1 which entails placement of gastroesophageal plications to create a partial anterior esophagogastric fundoplication above the Z-line.11 12 13
What About the LINX Procedure, Is It Any Better Than Having a TIF Procedure?
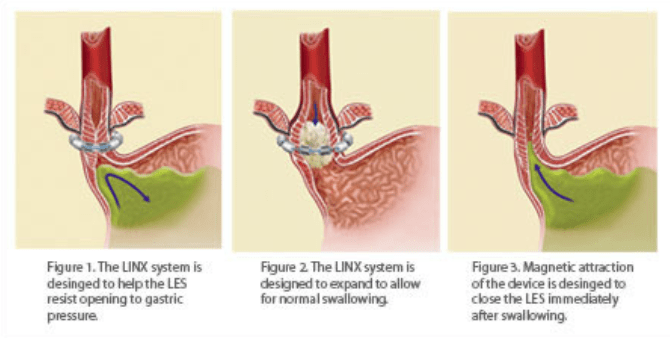
The TLDR is no, I believe the LINX procedure has more postoperative complications, and I do not recommend it. The LINX device was approved by the United States Food and Drug Administration in 2012 for GERD. The LINX device is a band composed of a string of ten or more beads containing a sealed core of magnetic neodymium iron boride, which is interlinked with independent titanium wires. The band is placed around the lower esophageal sphincter during laparoscopic surgery. The LINX band contracts and puts pressure on the lower esophageal sphincter at rest, keeping it closed and prevents reflux from entering into the esophagus. The band loosens its magnetic bound around the LES and expands when swallowing and allows the LES to open properly allowing swallowed contents to enter the stomach for digestion. The LINX device also loosens when the pressure in the abdomen becomes too great and will enable contents to exit the stomach like when belching or vomiting.14
Reported hospital stays are relatively short for the laparoscopic surgery, with discharge on either on a postoperative day or even as soon as the day of the operation. After the procedure, the patients are started on a diet early in the postoperative course even as early as surgery day to determine efficacy and complications of the surgery and device. Early introduction of food after the procedure may reduce the formation of a constrictive scar capsule around the band, which may lead to reduced dysphagia and proper healing. Patients who have the implant surgery should be made aware the LINX device may affect their ability to undergo magnetic resonance imaging (MRI) procedure. As per the LINX implant card, those with the device placed before May 22, 2015, may only be exposed to MR of 0.7 Tesla, while those with the device placed after may be exposed to MR of 1.5 Tesla. People with an implanted LYNX band might be at risk of the device heating up and causing internal burning and scaring if exposed to too strong of a magnetic field since the band is comprised of magnetized metals.15
Meta-studies show that the LINX is more effective than other anti-reflux surgeries for those who have the procedure performed and with fewer side effects:16
In 2015, Saino et al published the 5-year follow-up outcomes of the feasibility trail first reported in 2010. Thirty-three of 44 subjects were available for follow-up and 20 subjects completed esophageal pH testing. Total percentage of time with pH <4 was found to be 4.6%, still down from 11.9% (P<0.001). Seventy percent (14/20 subjects) achieved normalization of esophageal pH. The mean GERD-HRQL scores at 5 years improved further down to 2.9 from 25.7 (P<0.001). Complete cessation of PPI use was achieved by 87.8%. No patients had erosion or migration of the Linx device.
Ganz et al went on to publish the 5-year results of their pivotal trail of 100 patients in 2016. At 5 years, 85 patients were available for follow-up. The median GERD-HRQL score for these subjects dropped from 27 (off PPIs) to 4. PPIs were used by 100% of patients prior to the procedure and 15.3% of patients at 5 years. Fifty-seven percent of patients reported moderate-to-severe regurgitation preoperatively, while only 1.2% of patients have this complaint at 5 years. Bothersome dysphagia did increase with 5% reporting this symptom at baseline and 6% reporting it at follow-up. No patients lost the ability to belch or vomit when needed and no device erosions, migrations, or malfunctions occurred.
In a 2017 retrospective study of 170 patients who underwent MSA with the Linx device, excellent outcomes (GERD-HRQL <5) were reported by 47% of patients, good (GERD-HRQL 6–15) by 28%, fair (GERD-HRQL 16–25) by 22%, and poor (GERD-HRQL >25) by 3% of patients at median follow-up of 48 months. Review of patient characteristics revealed that a BMI >35 kg/m2, a structurally defective sphincter, and elevated residual LES pressure were frequently present in patients with less favorable outcomes of MSA.
There are some complications associated with the procedure, which include dysphagia (more common than a Nissen procedure), achalasia, esophageal spasm, tissue erosion, pain, nausea, vomiting, and scar tissue formation. Compared to laparoscopic Nissen procedures, the risk of “gas” bloat syndrome with the Lynx procedure is negligible, and fewer people had issues vomiting (4.3% compared to 21.3%). Costs for both procedures were similar (US$48,491 MSA vs US$50,111 Linx, P=0.506) and operative time was less for the LINX procedure (66 min MSA vs 82 min LNF, P>0.01). So what are studied statistics on the risk occurrences of LINX procedures?17 18
In Bonavina et al’s 2010 feasibility study of the Linx device, early dysphagia was the most common complaint, occurring in 43% of the patients. In most cases, this condition self-resolved by 90 days. During the 2-year period of the study, one device was laparoscopically explanted for persistent dysphagia. There were no reported device migrations, erosions, or related mucosal injuries. At the 5-year follow-up, there were still no device migrations or erosions reported.
In Reynolds et al’s 2014 publication, the most common complication was also dysphagia. This was seen in 82.7% of the 67 subjects, but resolved in 79% of these patients in a median time of 8 weeks. Eight of the patients experienced persistent dysphagia, which required balloon dilation. This led to improvement in symptoms in all patients. The second most common side effect was painful esophageal spasm, which was reported by 5.7% of patients.
Given the increasing awareness of complications that may warrant removal of the device, Asti et al published a review of this topic in 2017. At a median follow-up of 48 months, 11 of the 164 patients who underwent MSA had their Linx device explanted, usually between 12 and 24 months after surgery. Two devices were removed due to endoluminal erosion, while the rest were removed for dysphagia or recurrence of heartburn and chest pain.
Esophageal erosion appears to be the most significant complication of the Linx procedure. While rare, in the few case reports discussing erosion, the device was found to compromise the lumen of the esophagus and cause severe dysphagia. In discussions of eroding devices, the Linx device has been successfully removed without producing esophageal leaks or other long-term sequela. Of the literature reviewed, one case was identified in which the device was removed in a two-stage procedure: endoscopically using an Olympus Endoloop cutter to extract the eroding beads and later laparoscopically to remove the remainder. In the other cases, the device was able to be completely removed in one procedure either endoscopically or laparoscopically with no further intervention.
After reading those statistics, you might be asking yourself, why does John not recommend the LINX procedure over having a TIF? First, I do not endorse any of the anti-reflux surgical procedures if necessary because of the risks and side effects associated, but if you must have one performed TIF is probably the best. However, if you visit Facebook groups and boards dedicated to anti-reflux surgeries, you will discover that LINX tends to have way more complications including dysphagia, achalasia, and erosions then are reported in the efficacy studies. Furthermore, there is a rebuttal to the Ganz study on LINX procedures casting doubt on the safety of the procedure by Dr. Klaus Bielefeldt that shares similar reservations and beliefs that complications are probably underrepresented within the studies. I do not recommend the LINX procedure because I believe the overwhelming anecdotal evidence of issues associated with the LINX device outweighs any therapeutic potential of the surgery in healing reflux diseases. Finally, the LINX procedure does not address the root causes of a person suffering from reflux in the first place, like all antireflux surgical procedures.19
So What Can Be Done For Reflux Relief?
Since there are many different causes of reflux, there is not one protocol that will help you find relief. For some people, it can be a simple as taking D-limonene every other day for dinner for two weeks. For others, it can take months to relieve upper gut dysbiosis or small intestine overgrowth syndrome, two significant reflux causes. However, I would read the following linked blog article on the different types of reflux and how to find relief hopefully. Finally, listen to this Fix Your Gut podcast on reflux to gain more wisdom on how to improve your digestive health, work with an integrative health care professional in improving your digestive health, or contact me for coaching and let us resolve your reflux.
- Beers, Mark, The Merck Manual, Merck Research Laboratories, 2006 ↩
- Beers, Mark, The Merck Manual, Merck Research Laboratories, 2006 ↩
- https://www.sciencedirect.com/science/article/pii/S2255534X17300063 ↩
- Beers, Mark, The Merck Manual, Merck Research Laboratories, 2006 ↩
- http://www.hon.ch/OESO/books/Vol_6_Barrett_s_Esophagus/Articles/vol2/art023.html ↩
- Beers, Mark, The Merck Manual, Merck Research Laboratories, 2006 ↩
- https://www.sciencedirect.com/science/article/pii/S2255534X17300063 ↩
- https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4894777/ ↩
- https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3271216/ ↩
- https://www.ncbi.nlm.nih.gov/pmc/articles/PMC5390325/ ↩
- https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4894777/ ↩
- https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3271216/ ↩
- https://www.ncbi.nlm.nih.gov/pmc/articles/PMC5390325/ ↩
- https://www.ncbi.nlm.nih.gov/pmc/articles/PMC6124788/ ↩
- https://www.ncbi.nlm.nih.gov/pmc/articles/PMC6124788/ ↩
- https://www.ncbi.nlm.nih.gov/pmc/articles/PMC6124788/ ↩
- https://www.ncbi.nlm.nih.gov/pmc/articles/PMC6124788/ ↩
- https://www.cghjournal.org/article/S1542-3565(16)30167-7/pdf ↩
- https://www.cghjournal.org/article/S1542-3565(16)30167-7/pdf ↩




Hi John, I know the comment above was made more than a year ago, but as you made no reply, I have the same question for you. What are your thoughts on the Stretta procedure? I see that Dr Jamie Kaufman is now recommending that in her latest acid relief cookbook, whereas before she only recommended the Nissan fundoplication.
Thanks.
I’d really appreciate your input.
Not a fan as well I need to write about it.
Any opinion on Stretta procedure?