Roemheld Syndrome, What is it and How to Find Relief
Updated 2025
Roemheld syndrome (gastric-cardia syndrome) is personal to me. I know the condition exists even with the little information provided on the Internet to us about it. I suffered from it, and it caused me to have poor heart health for a time and arrhythmia.
I believe that the syndrome exists because I suffered from the syndrome after my son Abel died, and it was horrific.
My son Abel had passed away a month before I felt the dreaded symptoms of gastric-cardia syndrome. My silent reflux had come back in spades from all the stress. When I overate, my heart rate would suddenly dip, then shoot up to 150+ beats per minute. My blood pressure would also go sky-high. Why is this happening to me? I started to notice some patterns over time. When I drank water and burped, I felt better. When I took magnesium or had a bowel movement, I felt better. When I slowed my breathing and ate less, I also felt better. I did not know about gastric-cardia syndrome then, but I went on a restrictive low-FODMAP, Dropping Acid Diet. I also felt better. Both diets reduced microbial fermentation, bloating, and inflammation which relieved my symptoms. In a few months, I lost weight and got my digestion under control, and the symptoms went into remission.
Roemheld syndrome is well known in Germany, but not much of the medical condition is known outside of Europe. I hope I can spread awareness about this cruel, debilitating medical condition.
What Is Roemheld Syndrome and How Serious Is It for Your Heart Health?
Roemheld syndrome, also known as gastric-cardia syndrome and was discovered by the German medical internist Ludwig Roemheld in the 1930s. It is a condition where inadequate digestive health and/or microbial dysbiosis leads to cardiac symptoms and health issues. Have you ever felt your heart beat slow or very fast during or after eating a meal that was relieved by burping? Have you ever felt your heart skip for multiple beats or have chest pain after eating a large meal? You probably suffer from gastric-cardia syndrome.
Most of the following symptoms of the syndrome occur after eating, mainly if you consumed a large meal. Some people have also reported their symptoms after strenuous activity, when excessive pressure is applied to their abdomen, or when awoken with dyspepsia during the night.
Here are the proposed symptoms or consequences:
- Abdominal pain
- An abnormal amount of premature ventricular contractions (PVC’s). When PVC’s are occurring it feels like your heart is skipping beats.
- Anxiety
- Arrhythmia (heart palpitations)
- Atrial fibrillation
- Chest pain (angina pectoris)
- Cibophobia (fear of eating)
- Coughing and/or throat clearing
- Development or worsening of heart disease
- Depression
- Fatigue
- Facial flushing
- GERD (gastroesophageal reflux disease), silent reflux, bile reflux, or endotoxin reflux symptoms
- Hot flashes
- Hypotension
- Hypertension
- Insomnia
- Malaise (feeling of impending doom)
- Muscle cramps
- Muscle spasms (fasciculations)
- Poor sleep quality and frequent wakening
- Sinus bradycardia (less than sixty heart beats a minute)
- Sinus tachycardia (greater than one hundred heart beats per minute)
- Somniphobia (fear of sleeping)
- Sudden cardiac death (very rare)
- Supraventricular tachycardia
- Syncope
- Tinnitus
- Trouble breathing
- Weakness
- Vertigo
If you are showing symptoms of Roemheld syndrome, your healthcare professional will run tests to determine your cardiovascular health. A cardiologist might run the following tests to assess your heart health: an electrocardiogram, twenty-four-hour Holter monitor, cardiac scan (magnetic resonance imaging [MRI] or computed tomography scan [CT]), echocardiogram, and/or blood work. If your heart appears healthy, you might be referred to a gastroenterologist if you are also suffering from gastrointestinal issues. A gastroenterologist might also run a few tests to determine your gastrointestinal symptoms, including abdominal ultrasound, abdominal scans (CT, X-ray, MRI), and an endoscopy procedure. Most of the time, the only gastrointestinal issues found by the gastroenterologist in people suffering from Roemheld syndrome are reflux or a hiatal hernia.
Roemheld syndrome has a few mechanical triggers. A primary mechanical trigger of the syndrome occurs when excessive pressure is placed on the stomach’s fundus, moving upward and displacing its anatomical position. With increased epigastric pressure, the diaphragm’s position elevates and puts pressure on your heart, lungs, and vagus nerve. Hiatal hernias are a significant mechanical trigger of the syndrome and shift part of the stomach upward, putting pressure on your diaphragm, and causing breathing troubles. Gas produced from upper gut dysbiosis within the stomach can anatomically push the stomach upward from excessive bloating and distension. Finally, adhesions, anatomical surgical modifications, and meshes from gastrointestinal surgeries (including gastric bypass, hernia repair, and anti-reflux surgeries) may also displace your organs within the epigastric region, triggering gastric cardia syndrome.
“Hiatus hernia is associated with increased occurrence of GERD symptoms. Whether the presence of hiatus hernia further increase the risk of AF is unknown. A hiatus hernia as well as an intrathoracic stomach, representing the end stage of a hiatal hernial diaphragm, has the potential to mechanically irritate the left atrium. Additionally, the hernia may increase reflux and, thereby, result in oesophagitis accompanied by AF. The association between hiatus hernia and atrial tachyarrhythmias has been described as increases in atrial ectopic beats upon swallowing in a patient with a big hiatus hernia. Interestingly, there are case reports that repair of a large paraoesophageal hernia or an intrathoracic stomach can suppress paroxysmal atrial arrhythmias.“1
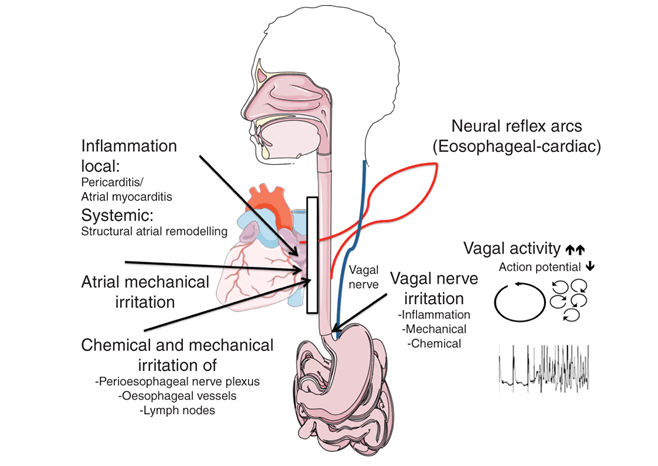
Another mechanical trigger of Roemheld syndrome is increased pressure on your vagus nerve. Your vagus nerve is your tenth cranial nerve that partly controls your autonomic nervous system. Your vagus nerve controls the parasympathetic nervous system response of your heart, lungs, and digestive tract. For example, gastrointestinal reflux can cause esophageal, throat, and laryngeal inflammation, which can cause increased pressure on your vagus nerve, interrupting its ability to properly transfer nerve impulses from your brain and other organs, including your heart and lungs. Heart rate and blood pressure may fluctuate widely when excessive force is placed upon your vagus nerve. Troubled and/or forced conscious breathing occurs when excessive force is placed upon your vagus nerve. When your heart rate and blood pressure drop, the body’s autonomic nervous system is activated by a catecholamine dump into your bloodstream, increasing your blood pressure and heart rate. The increased circulating catecholamines cause a massive increase in your blood pressure and heart rate and can cause panic attacks. Unless an underlying arrhythmia is triggered, the fluctuation from low to high cardiac pulses and pressure may be undetectable unless you are actively monitored during an attack; it can be easily mistaken as anxiety. Strong coronary reflexes happen when an attack occurs, causing many of the cardiac symptoms associated with the syndrome.
“Neural reflex arcs from the oesophagus and the heart have been shown in both animals and humans. In humans, chemical, electrical, and mechanical stimulation of the oesophagus modifies the sympathovagal balance. Oesophageal stimulation amplifies respiratory-driven cardiac vagoafferent modulation, while decreasing sympathetic modulation. Oesophageal acid stimulation is further associated with an increase in vagal activity.Acid refluxes cause a local inflammatory process that may directly alter the autonomic innervations of the oesophageal mucosa and may also penetrate the oesophageal wall and stimulate the adjacent vagal nerves. Injury of the distal oesophagus can further impair vagal nerve responses, particularly nerve sensitization of the afferent pathways. These and other considerations suggest the involvement of the cardio-oesophageal reflex in case of GERD associated AF.
Several observations support the relevant role of the autonomic nervous system for the initiation and the maintenance of AF. Studies in lone AF patients and in animal models of intermittent rapid atrial pacing and congestive heart failure have indicated that AF onset is associated with simultaneous sympathovagal activation rather than with an increase in vagal or sympathetic drive alone. On the cellular level, cholinergic muscarinergic receptors are the primary mediators of parasympathetic control of heart function. Muscarin-2 receptor (M2R) stimulation with acetylcholine directly activates G-protein-dependent potassium currents leading to a shortening of the atrial action potential duration and atrial effective refractory period.34 Additionally, the effect of vagal stimulation on atrial refractoriness is heterogeneous because of heterogeneity in the distribution of parasympathetic nerve endings and/or M2Rs. Increased vagal activation, as present in GERD-patients, creates an arrhythmogenic substrate for re-entry and, thereby, increases AF-susceptibility.“2
Excessive gas and bloating from dysbiotic flora in the small intestine and upper gut increases epigastric pressure, leading to the stomach moving upward, putting undue pressure on the vagus nerve, heart, and lungs, triggering gastric cardiac syndrome. Hydrogen, methane, and hydrogen sulfide production from fermentation by dysbiotic flora cause bloating, especially if one ingests a diet high in FODMAPs (fermentable oligo-, di-, monosaccharides, and polyols). Finally, obesity can also trigger Roemheld syndrome by increasing the risk of developing a hiatal hernia and cardiac issues.
“There is a 3–8% higher risk of new AF-onset with each unit increase in body mass index, and this association is independent of other cardiovascular risk factors. Pericardial fat is associated with the occurrence of AF, persistence of AF, left-atrial enlargement, and worse outcomes of AF ablation.44 Additionally, obesity results in progressive atrial structural and electrical remodelling. In sheep, following a high-calorie diet, obesity was associated with atrial electro-structural remodelling, increased atrial size, changes in conduction, and more persistent AF episodes. Obesity was associated with reduced posterior left-atrial endocardial voltage and infiltration of contiguous posterior left-atrial muscle by epicardial fat. Whether the anatomical proximity of the posterior wall of the left atrium and the oesophagus play a role for the development of this potential substrate for AF is unknown. In obese patients, risk factor management according to American Heart Association/American College of Cardiology guidelines improved the long-term success of AF ablation.“3
Roemheld syndrome RARELY causes heart disease and eventually heart failure. Over time, the syndrome may lead to a weakening of the cardiovascular system that might lead to cardiomyopathy and congestive heart failure from consistent arrhythmia and/or frequent sudden blood pressure changes.
Causes Include:
- Abdominal hernia and repair (mesh)
- Anti-reflux medication usage leading to upper gut dysbiosis (antacids, H2 antagonists, PPI’s)
- Being overweight or obese
- Celiac disease
- Excessive bloating and abdominal distension (SIBO, lactose intolerance, fructose intolerance, food intolerance, upper gut dysbiosis)
- Frequent antibiotic usage leading to upper gut dysbiosis
- Gas bloat syndrome (failure to burp)
- Gastric bypass surgery complications
- Hiatal hernia
- LES strengthening surgery complications (Nissen fundoplication, TIF, LYNX)
- Long-term physical and/or mental stress
- Poor liver, gallbladder, and pancreatic health
- Weakened LES (lower esophageal sphincter)
- Weight training (mainly from over-exertion of your core abdominal muscles)
What Can Be Done to Help Recover From Roemheld Syndrome
Here are some tips to help reduce your syndrome issues and improve your health:
- If a hiatal hernia causes your gastric-cardia syndrome, work on getting your stomach to remain in its correct anatomical position. Losing weight, primarily abdominal fat, might help reduce hiatal hernia symptoms. Chiropractic abdominal adjustments may help.
- Reduce stomach and intestinal tract bloating. If symptoms are severe, try a low FODMAP diet to reduce fermentation and bloating. Some people might need to reduce protein consumption to fifty grams daily it bloats you as well. Relieve SIBO or upper gut dysbiosis if you are suffering from it. Taking activated charcoal may reduce bloating from absorbing excess gas. Taking digestive enzymes may help reduce gas formation. Ensuring your stomach acid pH is optimal might help relieve upper gut bloating.
- Relieve constipation. Constipation can increase abdominal pressure, pushing the stomach upward causing Roemheld syndrome symptoms.
- Chew your food thoroughly and eat slowly. Do not overeat when full.
- To help prevent bloating, avoid consuming more than four to six ounces of beverages (including water) at your meals. Consume most of your daily beverages a few hours after a meal when your stomach is emptier. Avoid consuming carbonated beverages.
- If you are suffering from gastroparesis, try to improve your stomach emptying if possible. Consuming ginger tea hours after a meal or taking one New Chapter Ginger Force after a meal may help enhance stomach emptying.
- Activating your parasympathetic nervous system might help relieve Roemheld syndrome symptoms. I recommend grounding, praying to God the Father, humming, singing, omega-3 fatty acid ingestion, magnesium supplementation, proper sunlight exposure, proper sleep hygiene, and gargling.
- Avoid ingesting spicy foods and beverages, in which capsaicin ingestion partially inhibits parasympathetic nervous system activation from your vagus nerve.
- If you need to burp, try to make yourself burp by swallowing a little bit of water. Most of the time, burping relieves the symptoms of Roemheld syndrome.
- Exercise regularly to strengthen your cardiovascular system. Frequent walking seems to be an exercise that people with Roemheld syndrome easily tolerate. Supplement with magnesium and ubiquinol and maintain proper intake of dietary omega-3ids to help relieve heart arrhythmia. Avoid strenuous abdominal exercises or weight-lifting exercises that put pressure on your abdomen.
- Try to sleep on your back or side at all times if possible. Some people have fewer symptoms of Roemheld syndrome sleeping on their left or right side. Lying on your right or left side during an attack may provide instant relief. For most people, lying on the right side seems to help more, even if that is counterproductive to sleeping recommendations, for individuals who have GERD. Do not sleep or nap if you have eaten at least two hours before. If you do, it might be better to sleep in a recliner.
- Strengthen your diaphragm and improve your breathing!
- Strengthen your LES and UES (upper esophageal sphincter) tone if they are weak. Most people suffering from GERD have weak LES tone, and most people suffering from silent reflux have weak LES and UES tone.
- Try your best to lose weight if you are overweight to reduce increased abdominal pressure from excessive adipose tissue and to improve cardiovascular health.
Limited Resources
Information on gastric-cardia syndrome is limited, so if you find any relevant studies or books on the condition, please leave a comment below. Thank you.
Book:
- Enders, Giulia, Gut: The Inside Story Of Our Body’s Most Underrated Organ, Greystone Books, 2015.
Websites:
Podcast:
- Superhuman Radio #490 – Roemheld Syndrome
Studies:
Facebook Support Group:




The thirty symptoms symptoms or consequences of Roemheld syndrome has covered all the symptoms and signs of the issue.Thanks for sharing the article
I am a 36 year old male, a bit obese (5’11″/235 lbs). I have a history from age 16-30 of alcohol abuse, and cigarette smoking. Also abused cocaine from age 18-25. I have GERD and have been taking Omeprazole for 6 years now, 20mg once a day. I have been having a lot of PVCs/PACs for the past year, and they have really ramped up the past 6 months. I notice that when I get PVCs/PACs, my stomach will hurt and gurgle (gas). Also notice that my ear feels clogged and the left side of my neck descending from my ear is sore. I have a feeling that it is vagal nerve related. The PVCs/PACs have given me severe anxiety/panic disorder. I spent time in the US Army, and abused my abdominal muscles and back/neck. I need help, the PVCs/PACs are going to literally drive me insane. I think Roemheld could be the problem. I also notice that PVCs/PACs occur when I turn my head left or right or at the end of an exhale, right before I inhale. I take a lot of supplements like Ubiquinol, Magnesium, Selenium, D3, fish oil, NAC, Taurine/L-Arginine (I heard these two help arrhythmias, but it doesn’t seem to be helping), Liposomal Vitamin C, Quercetin with Bromelain, Inositol, K2, Astragalus Root, Apple Pectin, and to top it all off 15ml of Source of Life Gold liquid multivitamin. Please help me. Docs keep saying it is anxiety, but the PVCs/PACs are what is causing my anxiety. I feel like I am going to die soon.
Hi John – Reading your blog and then your book has been a life changer for me. After 4 gastroenterologists in 4 years and an extensive workup by my cardiologist, no one has been able to help me with the symptoms that you described for Roemheld syndrome. In fact when I mentioned Roemheld to my cardiologist, he totally rejected it. I decided to take charge of my own gut health and went on the low FODMAP diet. The improvement was amazing. I have just started following the constipation protocol in your books as I have been a lifelong sufferer.
My one question on the protocol is – how many days should I follow the guidance? Thanks!
Thank you for this wonderful space. My “theory” on my gastrocardiac syndrome for now (based on various research papers I read) is the following:
Excessive gastrointestinal distension – aggravated by indigestion, constipation, a blocked GI tract, SIBO, gut dysbiosis and /or other temporary/permanent conditions – causes excessive acid reflux as this is apparently an automatic response of the body.
No wonder many gastrocardiac patients feel that their GI tract is “stuck” and no wonder small spaced out meals, managing to burp, occasional fasting may help in some circumstances.
The excessive stomach acids manage to seap thru the esophageal tissue, which seems to be connected the vagus nerve endings (Bodur et al 2021). The situation is obviously aggravated if the esophagus /stomach area/GI tract in general is already inflamed due to intake of coffee, alcohol, chilli, chocolate, allergens, food causing intolerances etc. In fact, sometimes, gastrocardiac symptoms may be triggered by “wrong” food choices (allergenic/inflammatory) only.
When the innervation around the esophagus/heart area gets “triggered”, the heart electric signals go “out of balance” and various cardiac symptoms appear such as Afip, tachycardia etc (see Bodur et al 2021). The brain further perceives a sense of threat causing a very tough-to-control physical anxiety response, which further aggravates the symptoms; there’s plenty of evidence that anxiety is not simply “in the mind” (it can “subconsciously” manifest at the physical level). At the point, very little helps if not some deep breathing exercise and, in various circumstances, immediate medical attention.
The management of the conditions seems to be strongly related to a balanced diet, spacing out meals, increased intake of fiber (tough on IBS patient, who reportedly need to get used to this slowly), inflammation management, constipation management, allergy management, and gut flora management.
In brief, this gastrocardiac condition is complicated and multi factorial, and while physical anxiety in some patients may aggravate all, seeing it as the “root cause” doesn’t appear as a sound observation.
We have a telegram channel (see below); feel free to join for us to better describe our symptoms to physicians and researchers.
David F
https://t.me/+aEeyh8NmRacxOGEx
Great information in this video. https://www.beyondmthfr.com/mthfr-digestion-healing-hiatal-hernia/
There are a lot of things I lament about the internet, but posts and discussions like this reveal the true potential. Like others, I too have many of the symptoms listed. And like others, I too have been to the ER on several occasions, just to be told everything looks fine. Really? It doesn’t feel fine. Thank you for sharing this comprehensive information. You have given us insight that, in some cases, we’ve been seeking for years. Your efforts to help and educate are truly appreciated.
Some things I found that really help. Lift your arms up straight over your head to help get the gas out. Find out of you have a hiatal hernia and watch this video. I had immediate relief. I have severe debilitating Roemheld and this technique was a game changer. Medical professionals should all be doing this … watch and learn.
https://www.beyondmthfr.com/mthfr-digestion-healing-hiatal-hernia/
Some things I found that really help. Lift your arms up straight over your head to help get the gas out. Find out of you have a hiatal hernia and watch this video. I had immediate relief. I have severe debilitating Roemheld and this technique was a game changer. Medical professionals should all be doing this … watch and learn.
https://www.beyondmthfr.com/mthfr-digestion-healing-hiatal-hernia/
Hello, This blog is very useful
I had a paraesophageal hiatal hernia with most of my stomach up in my chest cavity pressing on my left lung and heart. I had robotic surgery with the stomach moved back in the abdomen and a LINX device placed around my esophagus.
Oh my goodness! My husband has been complaining about this for years. I believe him but everyone from his family thinks it’s all just in his head. Really hurts to see him suffer and we don’t know how to get a cure.
Find out of he has a hiatal hernia and watch the video in my post above. Best of luck.
Love your work – How do we connect verbally? I’d LOVE to speak to you about all this. Resonates so much with my own journey.
Godsend thank you
Have been dealing with this without diagnosis for years. I’ve had many an ER visit to only be sent away with valium and the prescription to calm down. My experience with this began about ten years ago after black mold poisoning which among many other effects disrupts the micro-biome and causes leaky gut and multiple food and chemical sensitivities. Again to John thank you so much for this information and I send love blessings and healing to every one of you here.
Recently started experiencing missing blood pulses after eating. I was able to record this on my smart phone using the finger pulse measuring with a special app. Currently awaiting Cardiologist’s report from a 24hr EKG.
I did some experiments to see what would trigger the gastric symptoms and the arrhythmia, and found that just trace amounts of food (e.g., Honey, Vinegar, etc.) dissolved in Water would be sufficient, and that the events would start within about 1/2 hour after swallowing and last for another 1/2 to 1 hour. By contrast, just drinking water would not cause any reactions. So, it seems that there may be other mechanisms than just pressure on the Vagus nerve, in Roemheld’s Syndrome. For example, a chemical mechanism involving: food causing digestive juices to be squirted into the duodenum, and then some of these juices somehow getting into the blood circulatory system, and affecting the heart.
Hey everyone! I’m 30 years old I’ve been sick now for 4 years. I’m diagnosed gastroparesis, hiatal hernia, GERD, silent acid reflux, reoccurring C-diff, gastritis., I’ve had my gallbladder removed. I have a lot of these issues with my stomach being linked to my heart. I always have heart palpitations PVCs mostly and sinus tachycardia. I’ve had two episodes where my heart goes crazy and shoots up to 160s with pressure in my chest and pain in my left arm I was convinced I was having a heart attack. I also had another episode in my cardiologist office while getting an EKG and it showed an elevated ST segment which resulted in my cardiologist sending me straight to the ER a medical team had to come and get me shortly before my episode I ate Mexican food because I knew I had the appointment and I wanted something to happen so he would believe me and boom it did. Food literally makes me sick. The gas pressure is unreal, the discomfort is unreal, the anxiety is unreal. I have dumping syndrome due to not having a gallbladder so sometimes before eating my blood sugar drops dangerously causing my pancreas to go into overload and my heart working in overtime trying to raise my blood pressure and I get dizzy and confused while on the toilet and fear that I’m going to die. Has anyone ever looked into FMT (fecal microbial transplant) to help with symptoms and improve gut flora? Just wondering. I know I have RS. I absolutely know,
I’ve been dealing with for five years now .. I believe I have leaky gut and trying to heal that now with my chiroprator and suppliments . But I had all the testing done with the heart doctor he said it’s normal I then went to gastric doc and he did scope down throat I have a small hernia and faulty gallbladder. Since having this I’ve done juice fasting for 30 days which made me feel great but I still had days where I had the heart skipping a beat. This is all started when I had a accident slipping and falling and getting a concussion I believe Vegas nerve was damaged . I’m now gonna start healing the leaky gut cause I believe it’s a direct connection and I’m gonna see a acupuncture to see if he can help the skipped beats. This is the year for healing for me I know it
Jami, How are you now?
Jami,how are you now?
Wow.i had ONE episode of rapid A Fib sending me to the ER. I have a history of GERD. 10-15 minutes before my heart doing flips, because I had just had a short lived virus, I thought I’d try coconut oil since I heard it is so good for you. I swallowed a tablespoon of it. I did nothing else unusual. BAM! Heart went crazy. When I got to the ER, I told them about the coconut oil. They looked at me like I was crazy and poo-pood the idea. I was put on a beta blocker. I began to notice little things… if I don’t eat regularly, I get pvc’s. If I’m constipated, chest discomfort. If I skip a meal , pvc’s. My ears ring all the time, sometimes louder than others and the pitch changes. I hate the beta blocker since it made me stupid. I want off it as I feel i have become dependent on it and fear what may happen if I go off. I have to see my cardiologist about this. I was so happy to hear about this syndrome. Could that be me?
Sounds like possibly Roemheld, talk to your doctor about it.
I have all of the roemweld symptoms you discuss. I was diagnosed with gastritis back in 2018. And have had months of knawing burning sensations in my stomach. That subsided then moved onto severe acid reflux and then just recently roemweld symptoms. I noticed last night I ate a little more than I’ve been eating lately…and the roemweld symptoms have not affected me for the last 13 or 14 hours. It might appear I have low stomach acid and the gastritis is the culprit
I get palpitations within minutes of eating almost anything. Im starting with digestive enzymes but i have many issues with medicine too and artificial sweeteners. Dairy and carbs are the worst.
Hi John,
Which type of magnesium is best RS? I found this article online (never knew there are so my different types of magnesium).
https://blog.bulletproof.com/best-magnesium-supplement/
What’s your advice?
Many thanks,
Rumy
So, I had a virus in Jan ‘17, which caused GERD. Oct ‘17 I developed Gastroparesis and SIBO. In April ‘18 The Gastroparesis seemed to subside, but I still have SIBO. For the past week, GERD and Silent Reflux have been acting up. I feel a sensation in my gut that travels to me chest. Today, after the sensation traveled to my chest, it caused my heart to jump. It happened twice this morning m, again an hour ago, and now I still feel like this heart feeling is looming. Does this sound like RS?
I have the exact same thing…not sure what else we can do but you’re not alone..oh and mine acts up worse from certain medications
Hmmm, this sounds like exactly what I have. Maybe this has nothing to do with it, but when I’m on the treadmill and wearing a heart monitor, I notice my heart rate slows down about 10-20 beats when I burp. I wonder if that establishes a connection between the gastro, vagas nerve, and cardio? And just like the symptoms say, I’ve had periods of bradycardia, tachycardia, dizziness, fatigue, light headiness, and more. Nothing ever shows up on the ekg or labwork. But it all started with gastro problems.
Sounds like Roemheld Syndrome to me.
Google Sanjay Gupta York Cardiology. Watch his videos, particularly the one on gastric-cardia. The guy is brilliant. Such a relief to find a doctor who does not scoff at this condition. It is clearly a VERY complex condition with a long list of triggers that vary person to person. Stress definitely is one or at least a contributor, but it is NOT a sole cause. Foods, drinks (caffeine, alcohol) are major contributors. You will need to carefully determine which you are more susceptible to. There is a lot of indirect research/info out there on food allergies and irritants which people with Roemheld clearly must be wary of. The important think is to rule out actual heart issues and then stop worrying about your heart and focus on the digestion, stress. Not much on it in the US, which is typical, since it is not a killer BUT Roemheld is REAL.
@Tony, thanks for discovering the Gupta videos. Not all of them are are his website http://yorkcardiologist.com/page6.htm — a lot of them are on YouTube and even at http://www.mashpedia.com/Roemheld_syndrome.
Sigh, would that all doctors had his ability (and willingness) to clearly explain medical concepts and conditions to patients. Thanks Dr G for providing these online videos!
I too have RS,that kicked in after my dad died.
Stress is a huge part of this. But when you have the weight of the world crashing down on your shoulders what do you do?
You slouch. Your breathing shallows out.
With my Rs I also noticed what could be described as esophagus twitching. On slouching,the esophagous is compressed. The vagus nerve is compressed,the gas in the gut is compressed. And pushes.
IMHO you cannot cure Rs without correct posture. Posture controls breathing.
Now, read this.
http://www.dpmartinjunghöfer.de/pdf/Breath%20Training%20for%20Roemheld%20Syndrome.pdf
Two years ago I became very ill, with constant episodes of sudden dizziness, heart pounding, hot flushing, etc. I did ER visits several times and they had no explanation. It all went away and now it’s back with a vengeance. I’ve had miserable Gerd, and I feel sure I have a hiatal hernia causing all this by pressing on my heart and vagus nerve, but I just had an endoscopy and they didn’t see the hiatal hernia. I’ve read it’s very easy to miss it, if it’s a sliding hiatal hernia. I’m 57, and 30 pounds over weight – mostly in my belly. I can’t stress enough that these episodes feels life threatening, and my heart pounds and then suddenly struggles to continue beating. My blood work up showed low b-12 and d, so I started supplements. I am scared and wonder if weight loss would help. I had a bad cold this week with hard coughing and I swear I can feel something laying along my esophagus on the right side.
How are you going now Diane?
Was referred to you from Bulletproof and came across this article. I’ve been Bulletproof for a few months with great benefits, but am burping quite a bit after morning coffee. I notice hot flashes after onions or fennel.
Now, thinking it might be Roemheld brought on by sibo, I am trying to limit fodmaps, but the grass fed butter, BP coffee, BP vanilla, and xct oil are all low fodmap, and I still burp after it.
I’m taking peppermint oil and probiotic, and it helps a little but not completely.
Should I eliminate the oil?
Go on a whey protein 3 day fast?
Thanks!
Peppermint can cause acid reflux…dont know if that is a problem but thought inwould mention…
Hiya, I have just discovered the condition ‘Roemheld syndrome’ and am wondering if i have it..
To cut a long story short, I have been feeling my heart stop followed by a sever dizzy spell followed
by a few heavy heartbeats with a head rush then back to normal, this happens when swallowing (food feels stuck, just before stomach) or burping for want of a better word!
I went to my Dr on more than 1 occasion and was always told to do more exercise
and sent for a ECG that always comes back normal…
I changed GP and when i mentioned these symptoms to my new Dr, she sent me for a 24 hour ecg monitor Thing! And after returning
the device I received a call from my GP asking me to come and collect report and go strait to Hospital :0
They discovered I get 3rd degree AV heart block lasting between 2 and 7.2 seconds!
I received a pacemaker but while I was in hospital to have the procedure I was hooked to an ECG Monitor for a few
days and could tell when the AV Heart block was about to happen… After I swallow food of burp… I mention this
to the cardio dr who said: “I cant stop you from swallowing food, you need this pacemaker.
Sorry for the long winded post but am wondering what you all think with re to my symptoms and ‘Roemheld syndrome’. I am due to see a gastro Dr for some further tests next week… I have already had a Endoscope (+6 biopsy’s) which all came back clear. On this visit i am to undergo a particular test that involves a tube being inserted into a nostril and down into my stomach which will then measure contraction of oesophagus? And a 24 hour acid monitor…. I am scared as nobody seems to believe me when I say that my Difficulty swallowing food AND 3rd degree AV Heart Block that I experience ARE INDEED LINKED. 100%
any thoughts will be very much appreciated
Thanks :)
I agree with you that you are probably suffering from Roemheld syndrome. I would look into uppergut overgrowth causing the issue like H. pylori, Citrobacter, or Proteus mirabilis. I would look into reducing uppergut overgrowth and maybe trying to test for it by getting a GI Effects test or http://biohealthlab.com/test-menu/parasites-and-pathogens/gi-pathogen-screens-401-401h/ for H pylori. I would talk to your doctor about taking magnesium and ubiquinol / PQQ for your heart and make sure your 25-hdroxy (vitamin D,) 1-25 hydroxy, and vitamin b12 levels are normal. Good luck!
Hi John
This sounds familiar to me. I think that I have experienced this on occasion, especially after going through two pregnancies in two years, which I know severely weakened my abdominal muscles (affecting the diaphragm)? When digestive health is optimal (zinc plays a big role in that for me), all is well. And, in fact, I can’t say that I’ve experienced this so much in the past couple of years. I have a slight abdominal bulge from the pregnancies that comes and goes (I had diastasis after both pregnancies. I’ve also noticed that it goes when my core is strong and my posture is correct), and I have had numerous people in healthcare positions tell me that it’s not a hernia. I don’t know, but i have seen it disappear and reappear with correlations to how I am feeling overall. My question is: would core strengthening exercises be helpful for this condition?
Thanks so much.
Hi John,
This sounds like me to a T. I’v seen 3 cardooglists and done almost every heart test short of a catheterization with no explanation for my chest pain, palpitations, shortness of breath and other symptoms. I do have a lot of upper GI symptoms including burping and bloating and will be seeing a gastroenterologist soon to check for a possible hernia or infection.
Hi there i would like to share a remedy for roemheld syndrome see if it can help..coz it has helped me to..take some black mustard seeds and dry roast them in a pan and as they start popping up put some water immediately and then filter this water removing the mustard seeds and drink this water..atleast one glass..
Hi Evan how are you going now, after 4 years? Would be great to hear from you! Thanks in advance.